Why Cutting Salt Is Dangerous If You Take Diuretics
Not everyone should cut salt. If you take a diuretic (often called water pills), reducing sodium too aggressively can cause serious health complications, needless to say most people are often never warned.
If you've ever been told to "eat less salt," you probably assumed that was universal advice. "Cut salt, protect your heart." Pretty simple, right? But for people taking diuretics, commonly prescribed for high blood pressure, heart failure, edema, and kidney disease, aggressively cutting salt can trigger a cascade of complications that are far more dangerous than the salt itself.
The One-Size-Fits-All Problem With Salt Advice
General dietary guidance recommends limiting sodium to 2,300mg per day (AHA guidelines). For most healthy adults, this is reasonable. But chronic disease management is not one-size-fits-all.
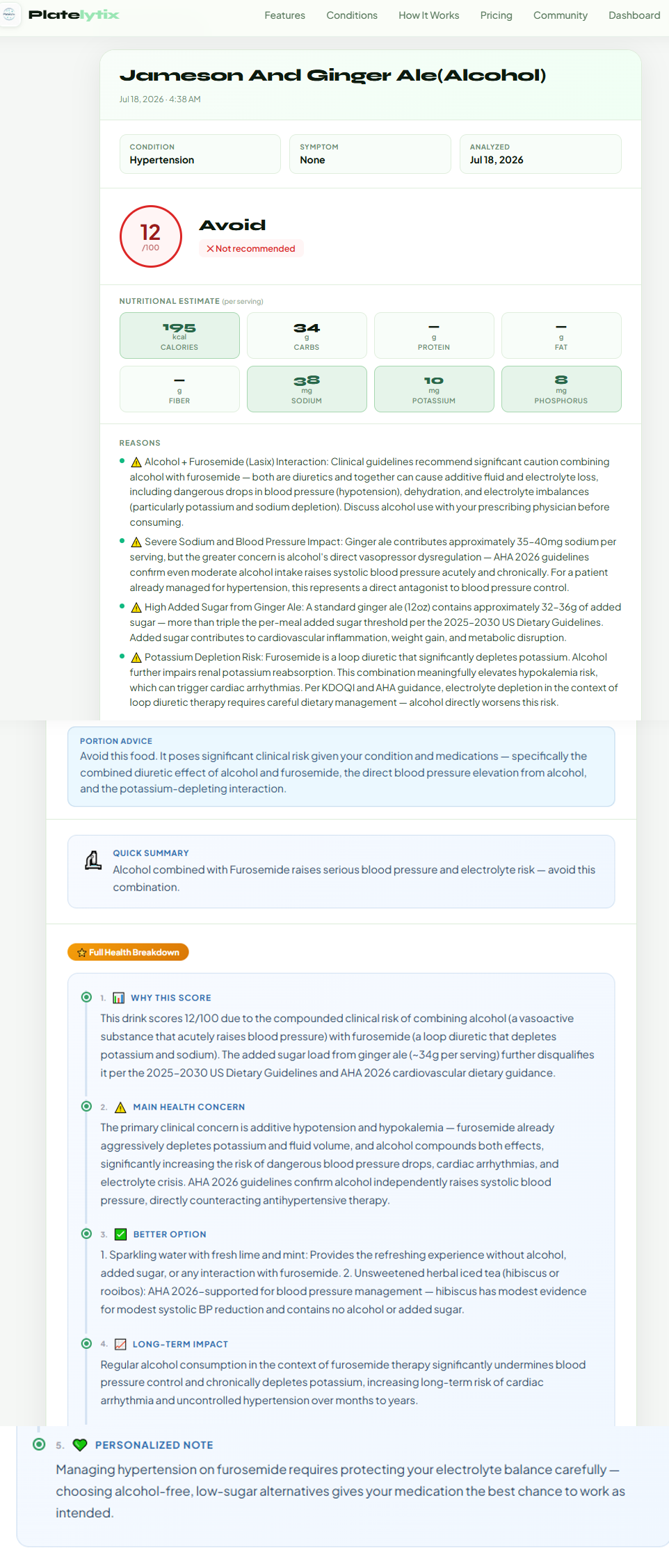
Diuretics (water pills) work by causing your kidneys to excrete more sodium and water through urine. Common diuretics include furosemide (Lasix), hydrochlorothiazide (HCTZ), spironolactone, and torsemide. When you combine these medications with an already low-sodium diet, you can push sodium levels dangerously low.
On a diuretic? See how your actual sodium intake scores against your specific medication and dose.
Score a Meal Free — No Account NeededWhat Is Hyponatremia — And Why It Matters
When blood sodium drops below 135 mEq/L, the condition is called hyponatremia. It is one of the most common electrolyte disorders in people on diuretics, particularly in older adults. Symptoms range from mild (nausea, headache, fatigue) to severe (confusion, seizures, coma, and in extreme cases, death).
⚠️ Many hyponatremia symptoms — brain fog, fatigue, muscle cramps — are easily dismissed as "just aging" or medication side effects. This means dangerously low sodium often goes undetected for weeks.
Symptoms of Hyponatremia (Low Sodium)
- Nausea and vomiting
- Headache and brain fog
- Fatigue and low energy
- Muscle cramps or weakness
- Confusion or difficulty concentrating
- Seizures (severe cases)
- Loss of consciousness (severe cases)
Who Is Most at Risk?
Heart failure patients
Often prescribed both a low-sodium diet AND loop diuretics like furosemide simultaneously. The combination requires careful sodium monitoring.
CKD (Chronic Kidney Disease) patients
Kidney disease impairs sodium regulation. NKF KDOQI 2020 guidelines emphasize individualized sodium targets — not blanket restriction.
Older adults on antihypertensives
Aging kidneys are less efficient at sodium conservation. Combined with HCTZ or similar medications, low-sodium diets can tip into deficiency rapidly.
People on thiazide diuretics
Thiazides specifically impair the kidney's diluting ability, making hyponatremia a documented risk even at moderate sodium restriction levels.
What Should You Actually Do?
This isn't an argument against sodium restriction. It's an argument for personalized sodium targets based on your specific medications, conditions, lab values, and kidney function. The right sodium level for you depends on:
- Which diuretic you take and at what dose
- Your current serum sodium level (from bloodwork)
- Your kidney function (eGFR)
- Whether you have heart failure, CKD, or liver disease
- Your fluid intake habits
CookGuide builds meals around your medical condition(s) and restrictions — calibrated to your labs, not generic advice.
Try CookGuideThis video encapsulates the argument for individualization of sodium control.
When Cutting Salt Becomes Dangerous — watch on YouTube.
Work with your physician or dietitian to establish your sodium target. Avoid generic internet guidelines. And if you are tracking your food intake, make sure your tool understands your health conditions rather than applying generic "low sodium" flags to everything you eat.
Set up your profile with your diuretic, dose, and labs, and get sodium targets calibrated to you — not a generic guideline.
Set Up Your Health Profile Score a MealDisclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult your nephrologist or renal dietitian before making dietary changes.
References: American Heart Association Sodium Recommendations (2021) · NKF KDOQI Clinical Practice Guidelines for CKD (2020) · Hyponatremia in Diuretic-Treated Patients, Journal of Clinical Medicine (2022)