What to Eat on Ozempic to Lose Weight (Without Losing Your Health)
Ozempic crushes your appetite. That's the point. But eating less of the wrong things accelerates nutrient loss, muscle wasting, and fatigue. Here's how to eat smarter — not just less.
The common mistake people make on Ozempic or any other GLP-1 drug isn't eating too much. It's eating too little of the right things.
Semaglutide (Ozempic, Wegovy) works by mimicking a gut hormone called GLP-1 (glucagon-like peptide-1) that signals fullness to your brain. It also slows gastric emptying — how quickly food leaves your stomach. The result is that most people on GLP-1 medications feel satiated on much smaller portions, sometimes eating half what they used to without trying.
That's the intended effect. The unintended effect is that when total food volume drops sharply, nutrient intake drops with it. A 2026 analysis published in Clinical Obesity reviewed data from 480,825 adults on GLP-1 medications and found that nearly 1 in 8 developed a measurable nutritional deficiency within just six months of starting treatment.
Of course, this isn't a reason to avoid Ozempic. It's a reason to be deliberate about what goes on your plate when you do eat.
See how your actual meals score for nutrient density, not just calories, on your GLP-1 prescription.
Score a Meal Free — No Account NeededWhy Food Quality Matters More on Ozempic, Not Less
Before GLP-1 medications, a nutrient gap in your diet could be partially compensated by volume — eat enough food overall and you'll likely hit most of your targets. On Ozempic, that buffer disappears. You might be eating one small meal and a snack and feeling completely full. If those meals aren't nutrient-dense, there's no cushion.
Semaglutide also slows gastric emptying, which means food sits in your stomach longer. This is why nausea is a common early side effect — and why heavy, fatty, or highly processed meals tend to feel particularly uncomfortable on the medication. Your food choices aren't just about nutrition; they directly affect how well you tolerate the drug.
What to Prioritize
Protein — Build Every Meal Around It
Approximately 40% of the weight lost on semaglutide comes from lean mass — muscle, not just fat — according to research presented at ENDO 2025 by Dr. Melanie Haines of Harvard Medical School. Women and older adults appear to be at the highest risk for disproportionate muscle loss.
Muscle matters beyond how you look. It regulates blood sugar after meals, supports bone density, and is directly linked to long-term metabolic function. Losing it while on a medication designed to improve metabolic health is counterproductive.
The clinical target most commonly cited for people on GLP-1 medications is 1.2–1.6 grams of protein per kilogram of body weight per day. For someone weighing 180 lbs (82 kg), that's roughly 98–131 grams of protein daily — across meals that are already smaller than before.
Best high-protein, low-volume options: Greek yogurt, eggs, cottage cheese, canned fish (salmon, sardines, tuna), edamame, chicken breast, and protein shakes when solid food feels like too much.
Platelytix meal score for a high-protein, low-volume meal on a GLP-1 profile
Vitamin D and Calcium — The Silent Pair
In a food-records study of GLP-1 users, 72% were consuming less calcium than recommended, and only 1.4% were meeting their daily vitamin D needs. These two nutrients work together — vitamin D is required for calcium absorption, so being low on one compounds the other.
Calcium doesn't cause acute symptoms when it drops. Instead, your body quietly pulls it from bone. Here's the mechanism: when blood calcium dips, the parathyroid gland releases extra parathyroid hormone (PTH), which signals bone to release stored calcium back into the bloodstream. Over time, this steady withdrawal from your "bone bank" becomes the real problem — measurable bone loss that often goes unnoticed until a fracture or a bone density scan reveals it.
Best sources: fatty fish (salmon, sardines with bones), fortified dairy or plant milks, Greek yogurt, bok choy, kale, and tofu set with calcium sulfate. Sunlight remains the most efficient vitamin D source, but dietary intake from fatty fish and fortified foods helps close the gap.
Iron — Especially If You're Female
GLP-1 users showed a 54% higher risk of low ferritin (stored iron) compared to people taking other diabetes medications. Uniquely, semaglutide appears to reduce intestinal iron absorption directly — not just through reduced food intake — based on prospective data published in Diabetes, Obesity and Metabolism.
Low ferritin often presents as fatigue and brain fog long before a standard blood count shows anemia. By the time anemia is visible on labs, the deficit has been building for months.
Best sources: lean red meat, organ meats, lentils, beans, fortified cereals, dark leafy greens. Pair plant-based iron with vitamin C (tomatoes, bell peppers, citrus) to improve absorption. Avoid coffee or tea within an hour of iron-rich meals.
Fiber — But Timed Carefully
Fiber is important for gut health, blood sugar regulation, and satiety. But on Ozempic, timing matters more than usual. Because gastric emptying is already slowed, a very high-fiber meal — especially combined with a large fluid intake — can worsen nausea and bloating.
The practical approach: distribute fiber across the day in moderate amounts rather than loading it into one meal. Oats, lentils, beans, berries, and cooked vegetables are gentler than raw cruciferous vegetables or high-fiber bars, which can feel brutal early in GLP-1 treatment.
Fluids — More Than You Think You Need
Appetite suppression also suppresses thirst signals for many people. Dehydration is underreported on GLP-1 medications and can amplify nausea, fatigue, and constipation.
Aim for consistent fluid intake throughout the day, not just when you feel thirsty. Water, electrolyte drinks (low sugar), herbal teas, and broth all count. If constipation is an issue, fluid intake is often the first lever to pull before adding a supplement.
Tubby and Frank on why "eating less" isn't the same as "eating right" on Ozempic — watch on YouTube.
What to Limit or Avoid
These aren't hard rules. They're foods that tend to worsen Ozempic side effects or crowd out nutrients you need:
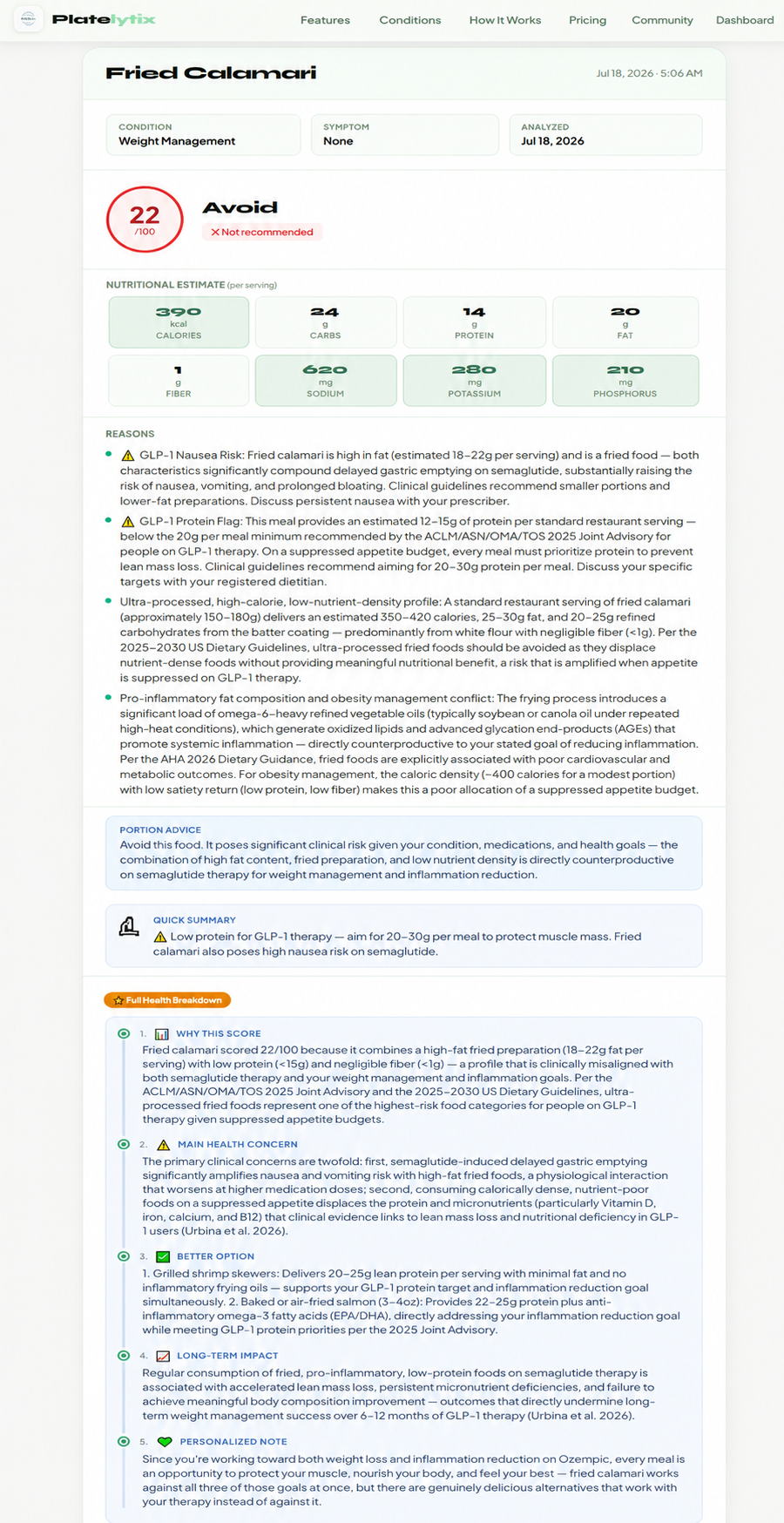
- Greasy or heavily fried foods — slow gastric emptying is already happening; adding high-fat meals on top dramatically increases nausea risk and delays absorption of fat-soluble vitamins.
- Ultra-processed snacks — low in nutrients, high in sodium and refined carbohydrates. On a reduced-calorie intake, every bite that doesn't deliver nutrition is a missed opportunity.
- Large portions in a single sitting — even of healthy foods. Ozempic changes the mechanics of your digestion. Several smaller meals or snacks spread across the day generally feel better than two large ones.
- Carbonated drinks — can worsen bloating significantly while gastric emptying is slowed.
- Alcohol — interacts poorly with blood sugar regulation and adds empty calories in a context where total intake is already limited.
Not sure what to make with what's nutrient-dense and GLP-1-friendly? CookGuide builds meals around your protein target, your medications, and your labs.
Try CookGuideA Sample Day of Eating on Ozempic
This isn't a meal plan. It's an illustration of what nutrient-dense, GLP-1-friendly eating can look like in practice:
Morning: Greek yogurt with berries and a small handful of walnuts. Coffee or tea, with water alongside.
Midday: A small portion of salmon or canned sardines over leafy greens with olive oil and lemon. A piece of whole grain bread or half a cup of lentils on the side.
Afternoon: A boiled egg or a small portion of cottage cheese if hunger appears. More water or an electrolyte drink.
Evening: Chicken breast or tofu with roasted vegetables (courgette, bell pepper, bok choy) and a small portion of quinoa or brown rice.
The goal isn't restriction on top of restriction. It's density — fitting the nutrients your body needs into the smaller eating window the medication creates.
See full recipes for meals like these — browse GLP-1-friendly recipes filtered to match your conditions and medications.
Browse RecipesIf You Have Other Health Conditions
Ozempic is frequently prescribed alongside other medications and alongside conditions that have their own dietary rules — CKD, heart failure, hypertension, GERD. Each of those conditions shifts what "eat well on Ozempic" actually means for you specifically.
Someone with CKD needs to balance protein intake (important for muscle preservation) against phosphorus and potassium load — a tension that doesn't exist for someone without kidney disease. Someone with GERD on Ozempic needs to be especially mindful of meal timing and portion size, since slowed gastric emptying can worsen reflux.
Generic "eat protein and vegetables" advice doesn't account for any of that. Your food choices need to reflect your full health picture, not just the medication you're on.
Why the Same Meal Scores Differently for Different People
Take the Evening meal from the sample day above: chicken breast or tofu with roasted courgette, bell pepper, and bok choy, plus a small portion of quinoa or brown rice. On the surface, it's a textbook healthy plate.
Here's what happens when that exact meal is run through Platelytix for two different people — both managing weight with Ozempic, but with very different health profiles.
Demo User 1 has no other diagnosed conditions beyond weight management. The meal scores 82/100 — Good. Platelytix flags the lean protein, the low-FODMAP vegetables, and the whole-grain carbohydrates as well-aligned with current dietary guidelines, with only a note about portion size given semaglutide's effect on gastric emptying.
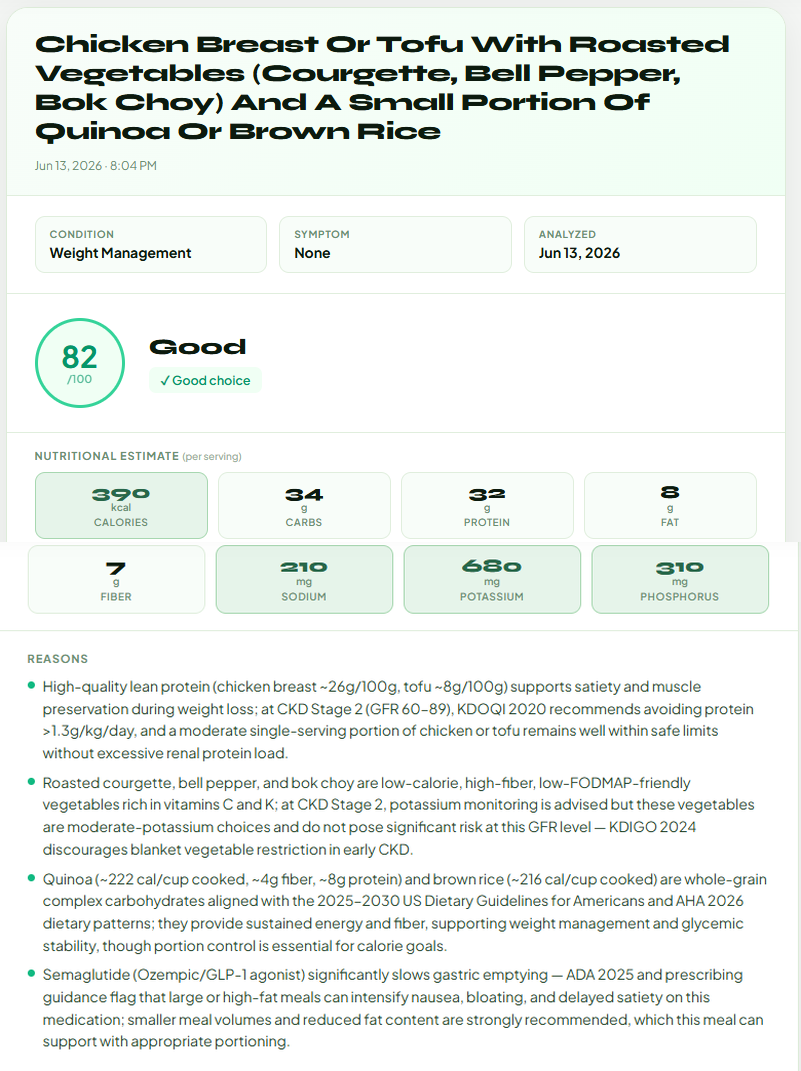
Demo User 1 — Weight Management only. Score: 82/100 (Good)
390 kcal · 34g carbs · 32g protein · 8g fat · 7g fiber · 210mg sodium · 680mg potassium · 310mg phosphorus
Demo User 2 has CKD Stage 2 (eGFR 68), hypertension, and obesity, and takes Lisinopril alongside Ozempic. The exact same meal scores 62/100 — Caution. Platelytix flags two things Demo User 1's results didn't need to consider: serum phosphorus already at 5.2 mg/dL (above the 4.5 mg/dL upper limit), with the quinoa and brown rice in this meal adding meaningful additional phosphorus load per KDOQI 2024. And serum potassium sitting at exactly 5.0 mEq/L — the upper boundary of normal — with Lisinopril (an ACE inhibitor) independently raising potassium, and the bell pepper, bok choy, and courgette in this meal each contributing potassium on top of that.
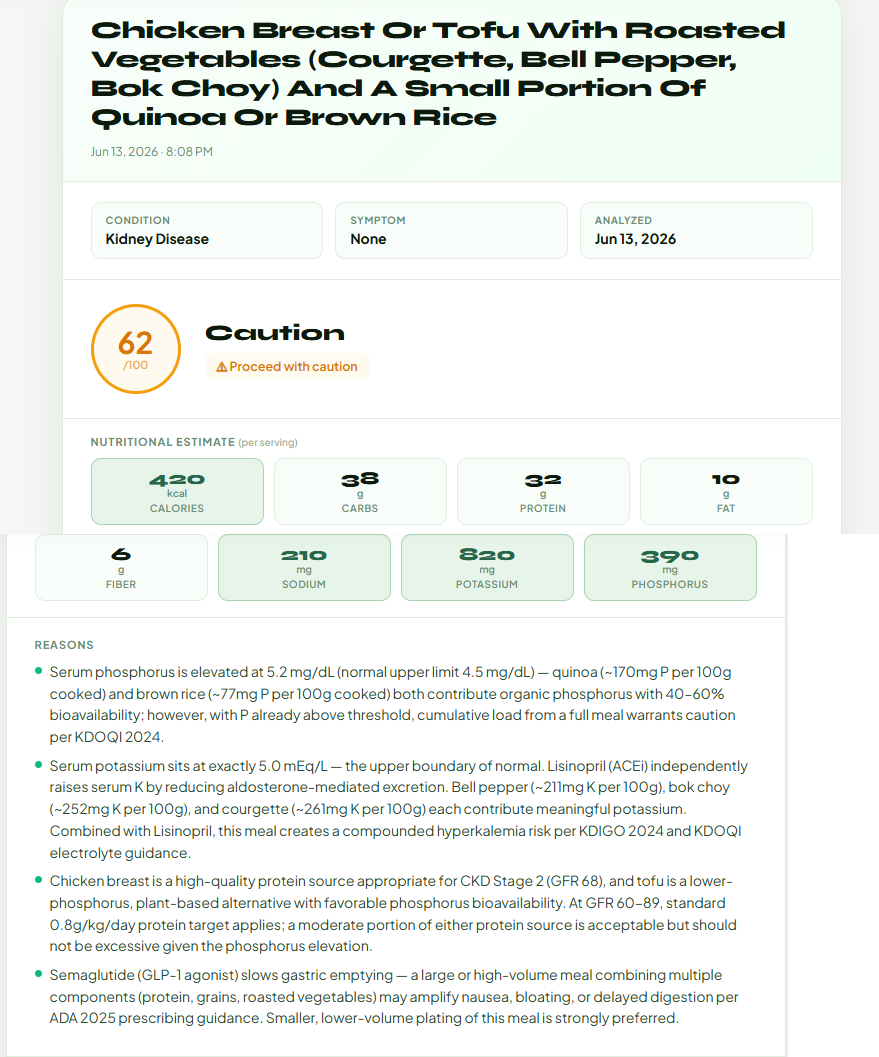
Demo User 2 — CKD Stage 2, hypertension, obesity, on Lisinopril. Score: 62/100 (Caution)
420 kcal · 38g carbs · 32g protein · 10g fat · 6g fiber · 210mg sodium · 820mg potassium · 390mg phosphorus
Same meal. Same calories, roughly the same macros. Two very different scores — because the meal itself is only half the picture. The other half is the person eating it.
This is the bottom line: a meal that's healthy and safe for one person may not be the same for another, based purely on their health status and recent labs. Generic nutrition advice — including most "what to eat on Ozempic" guides — can't account for this. Personalized guidance can.
Set up your health profile — conditions, medications, and labs — and see exactly how your meals score for you, not a generic user.
Set Up Your Health Profile Score a MealDisclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult your nephrologist or renal dietitian before making dietary changes.
- Urbina et al. Clinical Obesity, February 2026 — review of 480,825 GLP-1 users
- Haines M (Massachusetts General Hospital/Harvard Medical School). Semaglutide, protein intake, and lean mass. ENDO 2025 Annual Meeting, Endocrine Society
- Kushner P, Campos C, King A, Kruger DF, Morales J. "Clinician Guidance on the Benefits of Healthy Nutrition and Increased Physical Activity for People With Type 2 Diabetes Following GLP-1 Receptor Agonist Initiation." Clinical Diabetes, December 2025
- American Diabetes Association. Standards of Care in Diabetes — 2025
- Prospective iron absorption data: Diabetes, Obesity and Metabolism (semaglutide pilot study)
- National Kidney Foundation. KDOQI Clinical Practice Guidelines, 2020; KDIGO 2024 CKD Evaluation and Management Guidelines