Lisinopril and Potassium-Rich Foods: What You Actually Need to Know
The standard advice is "watch your potassium." Here's what that actually means — and the hidden source most people miss entirely.
If you take Lisinopril for blood pressure or heart failure, you've probably been told to be careful with potassium-rich foods. What most people don't get is why — or that the biggest risk isn't just bananas.
Why Lisinopril Raises Your Potassium
Lisinopril works by blocking the renin-angiotensin-aldosterone system (RAAS). One downstream effect: your kidneys excrete less potassium than normal. That's not a side effect you feel — it's invisible until your serum potassium climbs high enough to cause problems. The clinical threshold is 5.0 mEq/L. Above that, you're in hyperkalemia (high potassium) territory. Above 5.5, it's a cardiac risk.
It's worth noting that this isn't unique to Lisinopril. The same potassium-retention mechanism applies to every ACE inhibitor — Ramipril (Altace), Enalapril (Vasotec), Benazepril (Lotensin), Captopril, Quinapril (Accupril), and Fosinopril among others. If you're on any ACE inhibitor, the dietary guidance in this article applies to you equally. The same is true for ARBs — Losartan (Cozaar), Valsartan (Diovan), Olmesartan (Benicar), Irbesartan (Avapro) — which work on the same RAAS pathway and carry the same potassium-retention risk. Lisinopril is the most prescribed of the class, which is why it gets named specifically, but the interaction is a class effect, not a drug-specific one.
The Hidden Danger Most People Miss
The food risk most people hear about is bananas, oranges, potatoes. Those are real. But the single most dangerous source of potassium for Lisinopril users isn't a fruit or vegetable — it's salt substitutes.
Products like Morton Salt Substitute, NoSalt, and Nu-Salt replace sodium chloride with potassium chloride. They're aggressively marketed as heart-healthy. Many doctors recommend cutting salt alongside prescribing Lisinopril. The problem is that Lisinopril already reduces your ability to excrete potassium — and then a salt substitute floods your system with a concentrated dose of it. The combination can push serum potassium to dangerous levels faster than whole foods would. If you were told to reduce sodium and switched to a salt substitute, this matters for you specifically.
Foods and Products People Don't Think to Question
The bananas-and-potatoes list is where most articles stop. These are the sources that actually catch people off guard:
Coconut water — marketed heavily as a natural hydration drink and "heart healthy" electrolyte source. One cup contains roughly 600mg of potassium — more per serving than a medium banana. People on Lisinopril drinking coconut water after exercise are unknowingly stacking a significant potassium load on top of a medication already suppressing potassium excretion. There is a published case report of ascending paralysis from hyperkalemia in a patient on RAAS-blocking medication who was consuming coconut water regularly.
Sports drinks and "enhanced" waters — Gatorade, Powerade, and most electrolyte-fortified beverages contain potassium by design. The same goes for "mineral water" and enhanced sparkling waters. Always check the label for added potassium or electrolytes before assuming these are safe.
Dark chocolate and cocoa — 100g of dark chocolate contains over 700mg of potassium. A few squares isn't a crisis, but daily dark chocolate consumption — frequently marketed as heart-healthy — adds up fast on a medication that already retains potassium.
Molasses and blackstrap molasses — one tablespoon of blackstrap molasses contains roughly 300mg of potassium. It appears in health food circles as a mineral supplement, a natural sweetener, and a baking ingredient. Almost nobody warns patients on ACE inhibitors about molasses.
Tomato-based products — tomato paste, tomato sauce, ketchup, and canned tomatoes are significantly more concentrated than a fresh tomato. One cup of tomato paste contains over 1,000mg of potassium. Someone eating pasta with marinara or a home-cooked stew may be consuming far more than they realize.
Dried fruits — dehydration concentrates potassium dramatically. A quarter cup of dried apricots contains the same potassium as several fresh ones. Trail mix, granola bars, and "healthy" snack packs frequently contain dried fruit in portion sizes that add up quickly.
Lentils and beans — a cup of cooked lentils contains roughly 730mg of potassium. Legumes are frequently recommended as a heart-healthy protein swap — and they are generally beneficial — but portion size matters significantly on Lisinopril, especially when CKD is also present.
Potassium-fortified protein powders and meal replacements — many protein shakes, meal replacement bars, and electrolyte supplements add potassium explicitly as a selling point. Someone doing everything right nutritionally may be consuming an additional 200–400mg of potassium per serving from supplements alone, without realizing that the medication context changes everything.
Noni juice — specifically called out by NIH guidelines as a high-risk potassium source for ACE inhibitor users. Most physicians don't mention it because most physicians don't ask about it.
Who's Most at Risk?
The risk compounds significantly when other factors are present. Chronic Kidney Disease (CKD) reduces the kidney's ability to clear potassium independently of the medication. Diabetes affects aldosterone signaling. Age over 65 slows potassium excretion even in otherwise healthy kidneys. Being on spironolactone or another potassium-sparing diuretic alongside Lisinopril stacks the risk further.
A study of 5,171 CKD patients starting Lisinopril found a 90-day hyperkalemia risk of 2.8% overall — but 6.9% in the highest-risk group. That's not theoretical.
If you're managing CKD and diabetes alongside a blood pressure medication, the dietary conflicts run deeper — we cover that specifically in CKD and Type 2 Diabetes: What to Eat When You Have Both.
If you're managing both CKD and hypertension alongside Lisinopril, the dietary picture is more complex — potassium limits tighten significantly. These recipes are filtered for both conditions simultaneously:
What This Actually Means for Your Plate
This isn't a reason to avoid vegetables. The practical concern isn't any single food — it's the cumulative potassium load across your full diet, including the non-obvious sources above. The guidance is more targeted than a blanket restriction:
- Avoid salt substitutes containing potassium chloride unless your physician has explicitly cleared it with your current labs
- Keep high-potassium whole foods moderate and consistent — don't eliminate, don't binge
- Get your serum potassium checked regularly, especially if your diet or medications have changed
- Cooking method matters: boiling and draining vegetables reduces their potassium content by 30–50%
A Note on the Full Picture
Lisinopril doesn't exist in isolation. Most people taking it are also managing hypertension, CKD, diabetes, or some combination — each with their own dietary considerations that can conflict. The potassium guidance for Lisinopril is different from the potassium guidance for someone whose serum K is actually low, or for someone on a thiazide diuretic that depletes potassium.
Platelytix was built specifically for this kind of complexity — scoring foods against your full medication and condition profile simultaneously, not just one variable at a time.
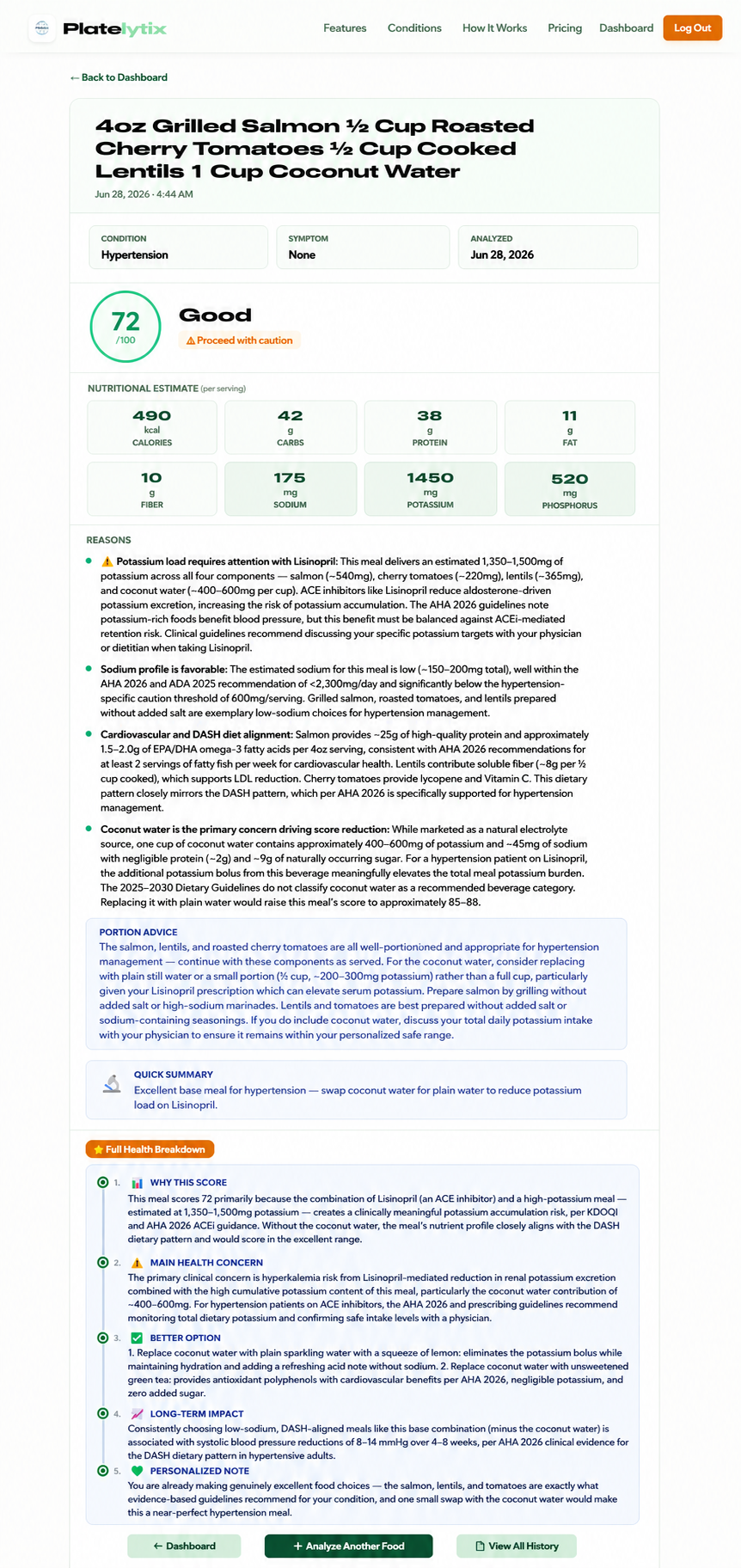
Below is a real Platelytix output for a user with hypertension on Lisinopril, run against a meal that looks healthy on the surface. The score isn't alarming — but the full health breakdown flags notable hyperkalemia risk based on current guidelines.
HTN-Friendly Meals That Work Around This
Managing potassium on Lisinopril doesn't mean giving up flavor or variety. The goal is building meals that are genuinely low in potassium stacking risk — not just "healthy" by general standards. Platelytix has a recipe library scored specifically for hypertension, with sodium and potassium already factored in.
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or registered dietitian before making dietary changes.